Informing Patients with a Rare Disease About Their Treatment Options
Despite the name, "rare diseases" affect 30 million Americans. Many of these conditions are debilitating, so the burden on individuals and families is substantial.

PCORI funds patient-centered comparative clinical effectiveness research (CER) studies that will provide more and better care options for people with rare diseases. Today, PCORI joins organizations around the world in recognizing Rare Disease Day to raise awareness of these conditions, their impact on patients and their families, and the research under way to improve care.
PCORI currently funds 23 research projects focused on rare diseases. Our work is guided by our Advisory Panel on Rare Disease, which includes patients, caregivers, advocates, researchers, insurers, life sciences industry representatives, and clinicians.
In one rare disease, lupus, the immune system attacks the body’s organs and tissues. This chronic disease can damage many parts of the body including the joints, skin, heart, and lungs. When the immune system attacks the kidneys, the disease is called lupus nephritis. It causes kidney damage and even end-stage kidney disease, which requires dialysis or a kidney transplant.
Over 300,000 Americans have definite or probable lupus. Approximately 50 percent of the patients will develop lupus-related kidney problems. Several medications are available to treat kidney disease in lupus, but it can be challenging to choose which medication is best for each person.
A PCORI-funded study on lupus nephritis is developing and testing a computer tool, called a decision aid, to help African-American and Hispanic patients with lupus nephritis make informed decisions. The project, should it prove helpful, might ultimately expand its focus to help patients with other conditions. We spoke with Jasvinder Singh, MBBS, MPH, of the University of Alabama at Birmingham, the principal investigator of the project, and Elyse Reyes, MPA, a patient partner on the study.
What do you want to accomplish with your study? Why focus on patients in minority groups?
Jasvinder Singh: Lupus affects young women much more than men or older women, and it’s more common and severe in racial and ethnic minorities. Minority patients tend to have worse outcomes. And around 50 percent or more of people with lupus will have kidney problems.
There’s also a lot of fear about immune-suppressing medications, but they’re hugely beneficial to controlling lupus and saving organs from damage.
We heard from patients that there was a need for materials that patients can understand. We are developing and testing a website to provide information to help them decide which treatments are best for them.
Elyse Reyes: The drugs are forms of chemotherapy medications. Even though they’re very mild compared to what you get for cancer, it’s a scary decision. You may vomit; you may lose your hair. That could mean time you have to take off from work, which you may not be able to afford. And the drugs are expensive.
I come from the Latino community. There’s a tradition there of deferring to the doctor without asking a lot of questions or getting much information. So the information patients do get tends to be from other people with the disease. It may or may not be correct. You hear worst-case scenarios and horror stories. The decision aid helps people get better informed.
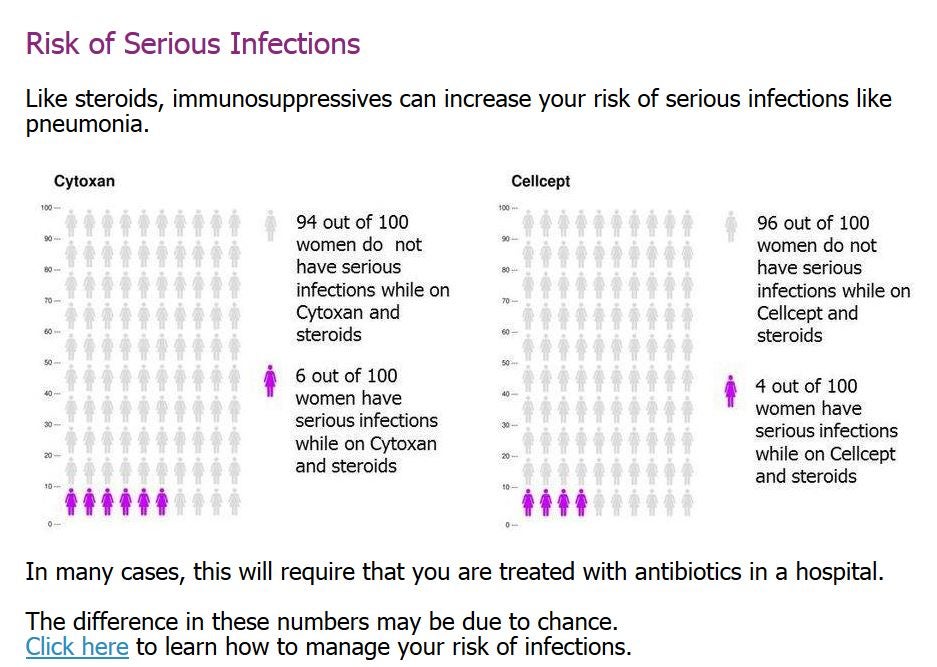
The decision aid helps patients understand the risks and benefits of various medicines for lupus. Shown is one page of the interactive web-based tool. (Courtesy of Jasvinder Singh; click image to enlarge)
How did you get involved in the study, Ms. Reyes?
Elyse Reyes: I was diagnosed with lupus in 2007. I moved from New York to Los Angeles, started a support group, and then got a job with Lupus LA, a nonprofit serving southern California. I created the patient programs there. It was my passion and my life’s work. In 2013, I had to resign because my own lupus flared. My disease is not focused on my kidneys. It’s been in my colon, which is not the most common manifestation.
Around that time, Jas Singh reached out. It was exciting for me to get involved in planning the research. When we started getting into the protocols for lupus nephritis, it turned out to be very similar to a treatment for my flare.
How do you think the decision aid might benefit patients?
Jasvinder Singh: We set up the online decision tool to provide information about the things patients cared about. If a lab test did not matter to patients, it did not show up in the decision aid. If hair loss mattered, it showed up on three pages.
Physicians are always excited about levels of creatinine (a marker of kidney function) and other blood tests, such as liver-function tests or white cell count. These are important. Nevertheless, we were more interested in comparing outcomes like uncertainty in decision making and informed choice among patients who do and don’t use the decision aid. The decision aid would have been a big zero if we did not have patients to tell us what to show, or more importantly, what not to show.
Elyse Reyes: The decision aid provides information in a way that’s easily accessible. It says, “This drug costs this much. These are some of the potential side effects.” It tells you to write down your questions. Then you can walk in to your doctor and say, “I’m worried about this, this, and this.”
I’ve always said my goal is to put myself out of a job. Every person should have the information they need.
The views expressed here are those of the authors and not necessarily those of PCORI.